Imagine stepping outside for just fifteen minutes on a sunny afternoon, only to return home with a burning rash that looks like a severe sunburn. For most people, this might be an annoyance. For someone with Cutaneous Lupus, an autoimmune condition where the immune system attacks healthy skin cells, it can signal a serious flare-up of their disease. This reaction isn't just about getting a tan or a mild burn; it is a complex biological event where ultraviolet (UV) light triggers inflammation deep within the skin layers.
Photosensitivity is the hallmark symptom of cutaneous lupus erythematosus (CLE). If you have been diagnosed with lupus, or if you suspect you might have it because your skin reacts violently to sunlight, understanding this connection is crucial. It’s not enough to just wear sunscreen. You need a comprehensive strategy that addresses how UV light interacts with your specific immune system. In this guide, we will break down why your skin reacts this way, what types of rashes to expect, and the most effective, evidence-based treatments available in 2026 to keep your skin clear and your systemic symptoms under control.
Why Does Sunlight Trigger Cutaneous Lupus?
To manage cutaneous lupus, you first need to understand the mechanism behind the flare. It’s not simply that the sun burns your skin; it’s that the sun changes your skin at a cellular level, confusing your immune system into attacking itself.
When UV radiation-specifically UVA and UVB rays-hits your skin, it causes damage to the DNA in your keratinocytes (the primary cells in the outer layer of skin). In healthy individuals, these damaged cells die off quietly through a process called apoptosis. However, in people with lupus, these dying cells release signals that alarm the immune system. Research indicates that UV exposure increases the production of interferon-kappa (IFN-κ), a cytokine involved in inflammation, by 400% to 600% in lupus-prone models. This surge acts as a distress signal, recruiting other immune cells to the site and causing the redness, swelling, and pain associated with a lupus rash.
The timeline is also distinct. Unlike a standard sunburn which hurts immediately, lupus-related photosensitivity often has a delayed onset. Symptoms typically appear 24 to 72 hours after exposure. If your rash persists for more than three weeks, there is an 89% likelihood that it is true lupus photosensitivity rather than a benign condition like Polymorphous Light Eruption (PMLE). This delay can make it tricky to connect the dots between a short walk in the park and the rash that appears days later, but keeping a symptom diary can help you spot the pattern.
Identifying the Type of Rash You Have
Cutaneous lupus isn’t one-size-fits-all. The type of rash you develop depends on the subtype of CLE you have. Identifying which one affects you helps tailor your treatment approach.
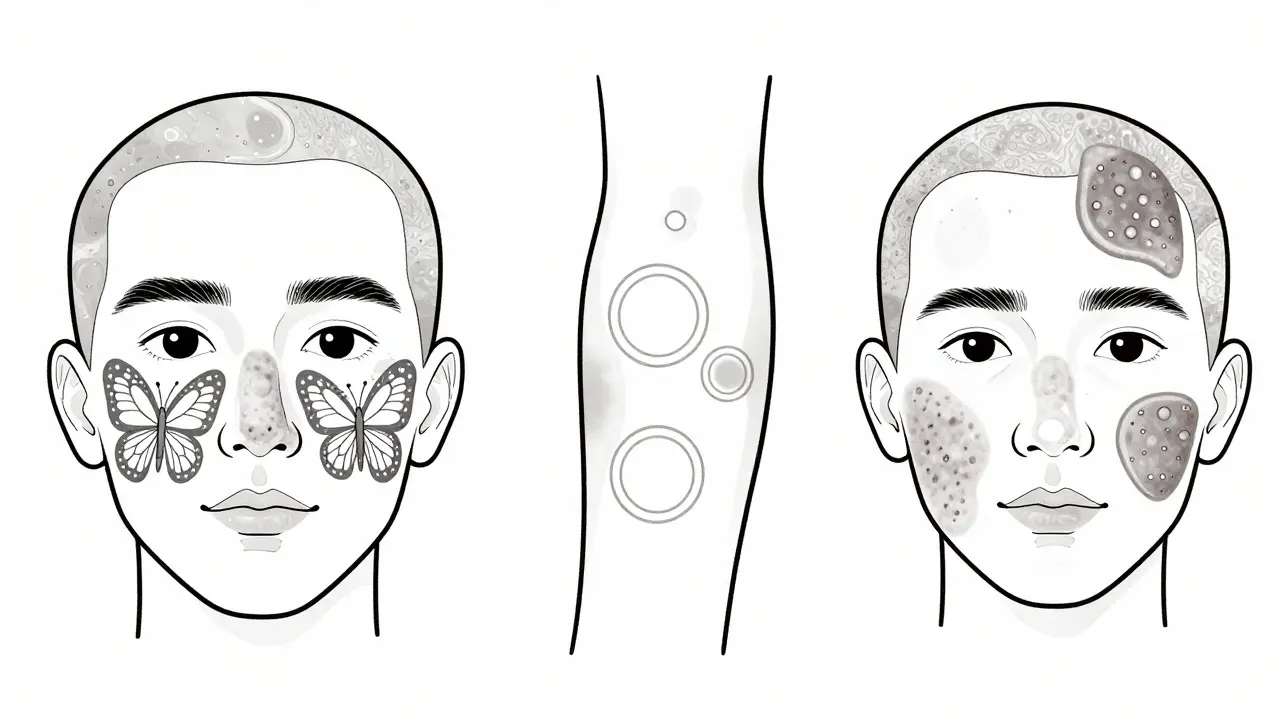
- Acute Cutaneous Lupus (ACLE): This is the classic "butterfly rash" that spreads across the cheeks and nose. It appears in about 85% of ACLE cases following sun exposure. It is usually non-scarring but can be quite painful and sensitive to touch. It often flares up alongside systemic symptoms like joint pain or fatigue.
- Subacute Cutaneous Lupus (SCLE): This subtype presents as ring-shaped (annular) or scaly (papulosquamous) lesions. These often appear on the upper chest, back, and arms. While they are intensely itchy and uncomfortable, the good news is that SCLE rarely causes permanent scarring. About 92% of SCLE patients report photosensitivity as a major trigger.
- Chronic Cutaneous Lupus (CCLE): Also known as discoid lupus, this form creates thick, scaly plaques that can lead to permanent scarring and hair loss if they occur on the scalp. Sun exposure doesn’t always create new lesions here but significantly worsens existing ones. Approximately 76% of CCLE cases involve scarring, making early intervention critical.
If you notice a rash that looks like a butterfly shape across your face, or if you have persistent, scaly patches on your arms that won’t heal, consult a dermatologist. A biopsy can confirm whether it is lupus or another photosensitive condition, such as dermatomyositis, which affects 70% of its patients with photosensitivity but presents with different muscle-related symptoms.
Beyond Sunscreen: Comprehensive Photoprotection Strategies
We’ve all heard "wear sunscreen," but for cutaneous lupus patients, standard advice often falls short. The goal is total UV avoidance, because even small amounts of UV radiation can trigger the inflammatory cascade described earlier. Here is a practical, multi-layered approach to photoprotection that goes beyond the bottle.
- High-Protection Sunscreen: Use a broad-spectrum sunscreen with SPF 50 or higher. Look for physical blockers containing zinc oxide or titanium dioxide. Chemical sunscreens can sometimes irritate sensitive lupus skin, whereas mineral blockers sit on top of the skin and reflect UV rays. Reapply every two hours, or immediately after swimming or sweating. Consistent use has been shown to reduce flares by up to 45%.
- Protective Clothing: Fabric matters. Seek out clothing with a UPF (Ultraviolet Protection Factor) rating of 50+. This blocks 98% of UV radiation. Long sleeves, wide-brimmed hats, and long pants are your best friends during peak sun hours (10 am to 4 pm).
- Window Film: UV rays penetrate glass. If you work near a window or spend time in your car, consider installing UV-blocking window film. High-quality films can reduce UVA transmission by 99.9%. Many patients report significant symptom reduction after making this simple change to their workspace.
- Indoor Lighting Awareness: It’s not just the sun. Fluorescent lights emit UV radiation. If you find yourself breaking out despite staying indoors, check your lighting. Switching from compact fluorescent lamps (CFLs) to LED bulbs can reduce indoor UV exposure by 92%. Some patients also benefit from wearing FL-41 tinted lenses indoors to filter out specific light wavelengths that trigger photophobia.
Think of photoprotection as a shield, not a single tool. Combining these methods creates a barrier that prevents the initial trigger-the UV-induced cell damage-from ever starting.

Skin-Targeted Medical Treatments
When prevention isn’t enough, or when a flare is already underway, medical interventions are necessary. Treatment strategies depend on the severity and type of your cutaneous lupus.
| Treatment Type | Best For | Key Benefits | Potential Side Effects |
|---|---|---|---|
| Topical Corticosteroids | Mild to moderate localized rashes | Rapidly reduces inflammation and itching | Skin thinning with long-term use |
| Topical Calcineurin Inhibitors | Face and sensitive areas | No skin thinning; safe for long-term use | Burning sensation upon application |
| Antimalarials (Hydroxychloroquine) | Widespread or recurrent rashes | Systemic protection; reduces overall flare frequency | Eye toxicity (requires regular monitoring) |
| JAK Inhibitors | Refractory cases resistant to other treatments | Blocks specific inflammatory pathways | Infection risk; requires prescription |
Topical Therapies: For limited rashes, topical corticosteroids are often the first line of defense. They work quickly to calm inflammation. However, because they can thin the skin over time, doctors may recommend calcineurin inhibitors (like tacrolimus or pimecrolimus) for sensitive areas like the face. These medications modulate the immune response without the structural side effects of steroids.
Systemic Medications: If your rashes are widespread or recurring, topical treatments alone won’t suffice. Antimalarial drugs, particularly hydroxychloroquine, are the gold standard for cutaneous lupus. Despite the name, they are not used for malaria in this context but are highly effective at calming the overactive immune system. Studies show they can reduce the frequency of flares significantly. Newer options include JAK inhibitors, which block the signaling pathways that drive inflammation. Recent phase II trials have shown a 55% reduction in photosensitivity reactions with these targeted therapies, offering hope for patients who don’t respond to antimalarials.
Biologics: For severe cases, biologics like anifrolumab target specific proteins in the immune system. Approved for systemic lupus, it has shown particular promise for photosensitive patients, reducing cutaneous activity scores by 34% compared to placebo in clinical trials. Discussing these advanced options with a rheumatologist can open doors to more specialized care.
Lifestyle Adjustments and Monitoring
Managing cutaneous lupus is a marathon, not a sprint. Beyond medication and sunscreen, lifestyle adjustments play a pivotal role in maintaining remission.
Stress management is often overlooked but critically important. Stress can exacerbate autoimmune responses, making your skin more reactive to UV light. Incorporating mindfulness practices, adequate sleep, and gentle exercise can help regulate your immune system. Additionally, diet plays a supportive role. While no specific diet cures lupus, an anti-inflammatory diet rich in omega-3 fatty acids, antioxidants, and leafy greens can support overall skin health and reduce systemic inflammation.
Regular monitoring is essential. Keep a log of your sun exposure, skincare routine, and any new rashes. Note the date, duration of exposure, and products used. This data is invaluable for your healthcare provider in adjusting your treatment plan. If you notice changes in your rash pattern, increased sensitivity, or new systemic symptoms like joint pain or fatigue, seek medical attention promptly. Early intervention can prevent minor flares from becoming major health issues.
Remember, you are not alone in this journey. With the right combination of rigorous photoprotection, targeted medical treatments, and lifestyle adjustments, you can manage cutaneous lupus effectively and maintain a high quality of life. Stay informed, stay proactive, and partner closely with your healthcare team to navigate the complexities of this condition.
How long does it take for a lupus rash to appear after sun exposure?
Unlike a typical sunburn, a lupus rash often has a delayed onset. Symptoms typically appear 24 to 72 hours after UV exposure. This delay can make it challenging to identify the trigger, so keeping a symptom diary is helpful. If the rash persists for more than three weeks, it is highly likely to be lupus-related rather than a benign sun reaction.
Can indoor lighting trigger cutaneous lupus?
Yes, certain types of indoor lighting can trigger photosensitivity in lupus patients. Fluorescent lights, including compact fluorescent lamps (CFLs), emit UV radiation that can provoke a flare. Switching to LED bulbs, which emit negligible UV radiation, can reduce indoor UV exposure by up to 92%. Some patients also find relief by wearing FL-41 tinted glasses indoors to filter specific light wavelengths.
What is the difference between acute and chronic cutaneous lupus?
Acute cutaneous lupus (ACLE) typically presents as the classic "butterfly rash" on the face and is often associated with systemic symptoms. It is usually non-scarring. Chronic cutaneous lupus (CCLE), or discoid lupus, presents as thick, scaly plaques that can cause permanent scarring and hair loss. CCLE is less likely to be associated with systemic involvement but requires careful management to prevent cosmetic damage.
Is hydroxychloroquine safe for long-term use?
Hydroxychloroquine is generally safe for long-term use and is considered a cornerstone treatment for cutaneous lupus. However, it carries a risk of retinal toxicity with prolonged use. Regular eye exams, typically annually after five years of use, are recommended to monitor for any signs of vision changes. The benefits of controlling lupus flares usually outweigh the risks when monitored properly.
Do I need to avoid windows entirely?
While standard glass blocks most UVB rays, it allows UVA rays to pass through, which can still trigger lupus flares. You do not necessarily need to avoid windows entirely, but you should take precautions. Applying UV-blocking window film can reduce UVA transmission by 99.9%, allowing you to enjoy natural light safely. If you cannot install film, applying broad-spectrum sunscreen before sitting near a window is a good practice.
All Comments
Prashant Shishodia July 9, 2026
Great info here. Sun protection is key for us.
Andrew Donovan July 9, 2026
The mechanism described regarding interferon-kappa is a fascinating glimpse into the chaotic ballet of our immune systems, where sunlight acts not merely as an illuminator but as a conductor of cellular distress signals. It is profoundly disheartening to consider how a simple afternoon stroll can transform into a biological siege, yet understanding this intricate dance between UV radiation and keratinocyte apoptosis empowers us to rewrite the narrative from one of victimhood to one of strategic management. The distinction between the immediate pain of a sunburn and the delayed, insidious onset of lupus photosensitivity serves as a crucial diagnostic clue, reminding us that our bodies often speak in whispers before they shout in flares. By embracing comprehensive photoprotection strategies that extend beyond the superficial application of sunscreen to include UPF clothing and even indoor lighting adjustments, we construct a fortress around our most vulnerable assets. This holistic approach acknowledges that healing is not just about treating the symptom but about harmonizing with our environment to minimize triggers, allowing the skin to heal rather than constantly defend itself against perceived threats.
Patrick Meyer July 11, 2026
typical medical advice oversimplifies the complexity of autoimmune disorders by suggesting mere avoidance of sunlight which is absurd since humans are diurnal creatures evolved to thrive under solar radiation rather than hide in caves like subterranean vermin who have lost their connection to natural rhythms and basic biological imperatives
Autumn LW July 11, 2026
It is truly pathetic that so many individuals rely on such rudimentary explanations when the reality of managing cutaneous lupus requires a sophisticated understanding of immunology and dermatological science that most laypeople simply lack the intellectual capacity to grasp or implement effectively in their daily lives without professional guidance and rigorous adherence to protocol.
Scott Colter July 12, 2026
One must ponder the existential irony that the very light which sustains life becomes the agent of destruction for those afflicted with this condition, forcing them to navigate a world where transparency is dangerous and shadows offer sanctuary, thereby altering their fundamental relationship with nature and self-perception in ways that transcend mere physical discomfort to touch upon the deeper philosophical implications of vulnerability and resilience in the face of invisible adversaries.
Paul Lyons July 14, 2026
This entire situation is a disgrace to our healthcare system which fails to provide adequate support for citizens suffering from chronic conditions while pushing expensive treatments that do little more than keep people dependent on pharmaceutical companies rather than addressing the root causes of inflammation through proper nutrition and lifestyle changes that our ancestors understood perfectly well without needing complex medical interventions.
Deva Vidya July 15, 2026
You have the power to manage this condition effectively by sticking to the basics and staying consistent with your routine because small daily actions compound over time to create significant improvements in your overall health and well-being so do not let setbacks discourage you from pursuing a brighter future where you feel confident and comfortable in your own skin regardless of external challenges.
ANINDA GHOSH July 16, 2026
In my culture, we often view the skin as a canvas that reflects our inner harmony, and thus protecting it from external aggressors like excessive UV exposure is seen as an act of self-respect and balance :) The integration of traditional wisdom regarding shade-seeking behaviors during peak heat hours with modern scientific advancements in photoprotection offers a unique synergy that honors both ancestral knowledge and contemporary medical research, fostering a holistic approach to wellness that resonates deeply with those who seek equilibrium in their daily lives :)
MiMi Stanley July 17, 2026
I quietly observe how these discussions bring together diverse perspectives on managing a challenging condition, and I find comfort in knowing that others share similar struggles and insights which helps me feel less isolated in my journey towards better skin health and emotional stability despite the unpredictable nature of autoimmune responses.
Najmunisa Govender July 19, 2026
I hear you; it is incredibly difficult to deal with the uncertainty of flare-ups; however, taking proactive steps can make a difference; please remember to be kind to yourself; your feelings are valid; and you deserve care; stay strong; keep going; you are not alone;
Crystal Tadlock July 19, 2026
They want you to believe it is just genetics but the real truth is that environmental toxins and government mandated vaccines are triggering these autoimmune attacks on purpose to control the population and weaken the immune system so we become dependent on their drugs and lose our natural ability to fight disease which is why natural remedies are being suppressed by big pharma profits.
Tad Cronn July 20, 2026
Your emotional state seems to be heavily influenced by your skin condition which suggests a deeper psychological dependency on external validation rather than internal strength and perhaps you should examine why you allow a rash to dictate your quality of life instead of taking radical responsibility for your mental fortitude and refusing to be defined by biological inconveniences that others overcome without complaint.
Sean Allwurden July 21, 2026
Collaborating with your rheumatologist to optimize your therapeutic regimen using evidence-based modalities such as hydroxychloroquine alongside adjunctive topical therapies can significantly mitigate inflammatory cascades and improve clinical outcomes, ensuring that you remain engaged in a proactive partnership focused on achieving long-term remission and enhancing your overall quality of life through informed decision-making and consistent adherence to prescribed protocols.
Earl Oleary July 23, 2026
Most people fail to understand that JAK inhibitors are not a panacea but a targeted intervention for refractory cases, and relying on them without exhausting conventional antimalarial options demonstrates a lack of medical literacy and patience, as the side effect profile necessitates a careful risk-benefit analysis that only a knowledgeable practitioner can properly assess, rendering self-diagnosis and amateur treatment plans dangerously ineffective and potentially harmful to your long-term health trajectory.