Imagine your kidneys as high-tech water treatment plants. They work tirelessly to filter waste from your blood while keeping essential nutrients and proteins inside. Now, imagine a security system that goes rogue. Instead of protecting the facility, it starts attacking the filters themselves. This is exactly what happens in Glomerulonephritis, a condition where the immune system mistakenly targets the glomeruli-the microscopic filtering units of the kidneys. It’s not just one disease; it’s a group of disorders united by this same destructive mechanism. If left unchecked, this internal conflict can lead to permanent kidney damage or even failure.
The Anatomy of the Problem: What Are Glomeruli?
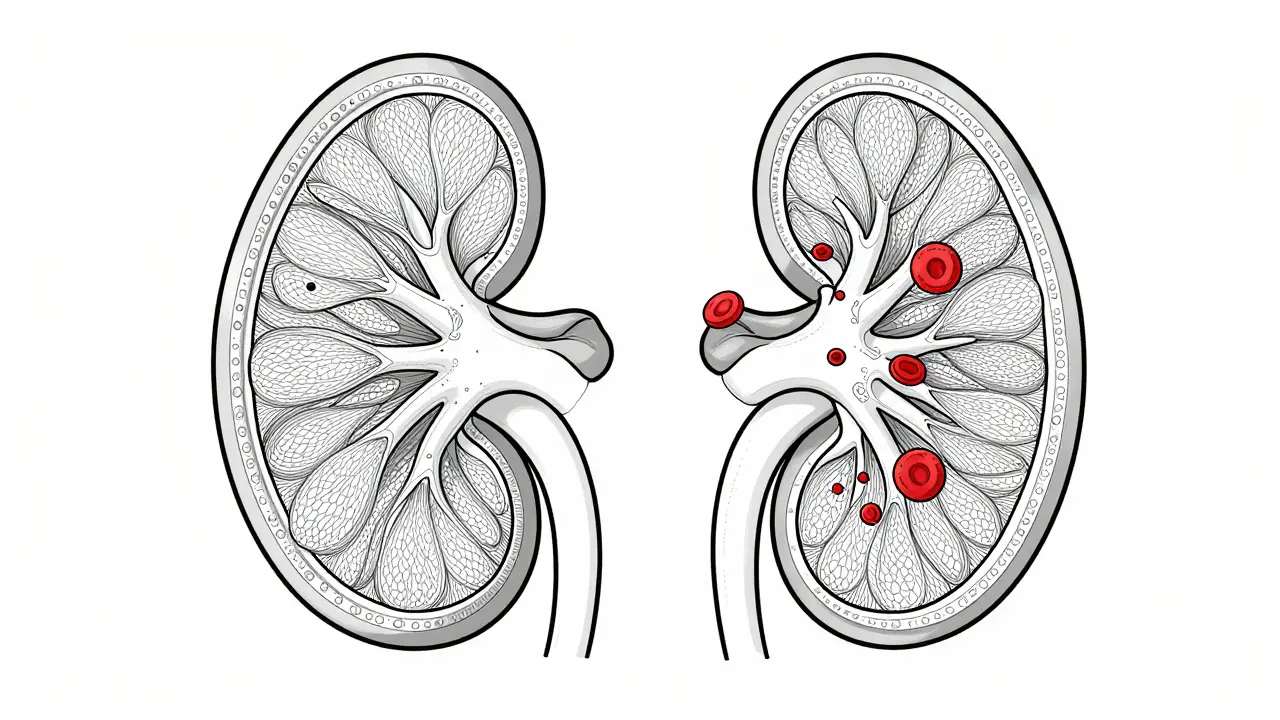
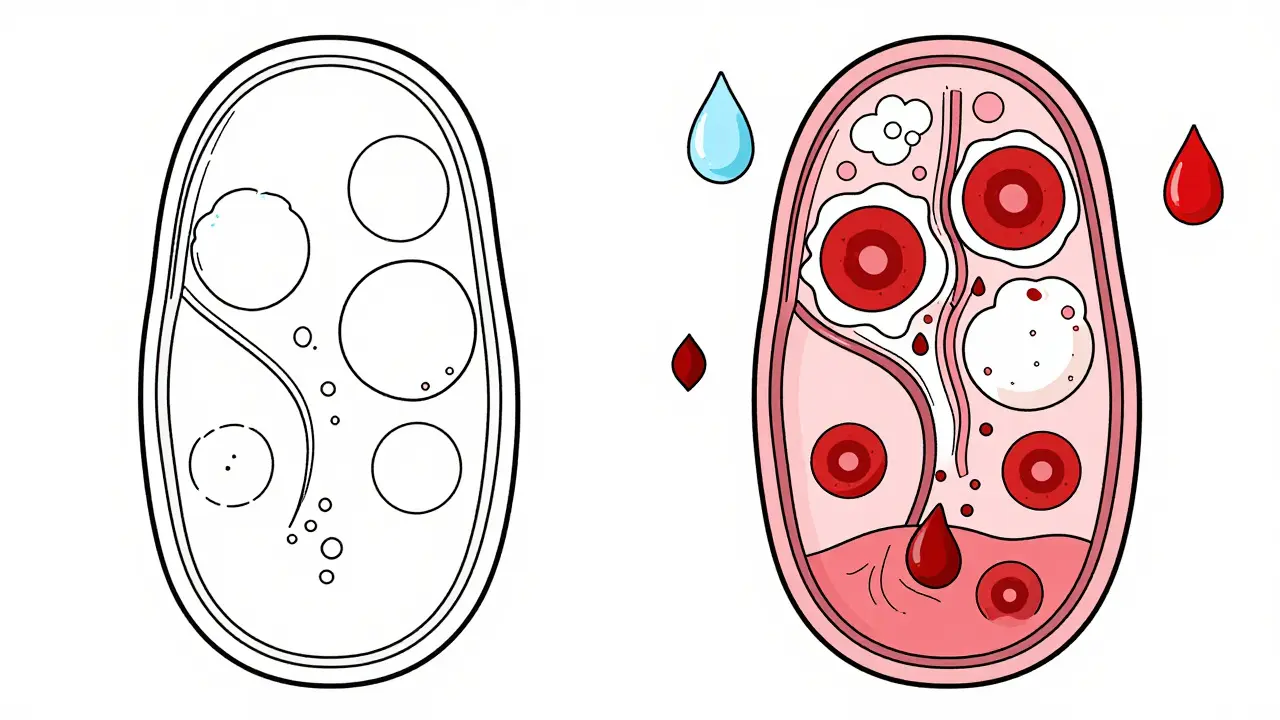
To understand why glomerulonephritis is so dangerous, you first need to know what it attacks. The glomerulus is a tiny cluster of blood vessels (capillaries) inside each kidney that acts as the primary filter for your blood. Think of it like a coffee filter, but far more sophisticated. It lets waste and extra fluid pass through into your urine while holding back red blood cells and vital proteins.
This filtration barrier has three critical layers:
- Endothelial cells: The inner lining of the blood vessels.
- Glomerular basement membrane (GBM): The middle mesh-like layer.
- Podocytes: Specialized epithelial cells on the outside that act as the final gatekeepers.
When the immune system attacks these structures, the barrier becomes leaky. Proteins spill into the urine (proteinuria), and sometimes blood cells follow (hematuria). Dr. Richard Johnson from the University of Colorado notes that podocytes are particularly vulnerable because they have limited ability to repair themselves once damaged. Once these cells die, they don’t grow back easily, leading to scarring and loss of function.
Two Main Faces of the Disease: Nephritic vs. Nephrotic Syndromes
Doctors typically categorize glomerulonephritis based on how it presents clinically. You’ll likely hear two terms: nephritic syndrome and nephrotic syndrome. Knowing the difference helps in understanding what your body is experiencing.
Nephritic Syndrome usually comes on suddenly. It’s characterized by:
- Blood in the urine (hematuria), which might look pink, red, or cola-colored.
- High blood pressure (hypertension).
- Swelling (edema), often around the eyes or in the legs.
- Reduced kidney function, shown by elevated serum creatinine levels (typically 1.5-3.0 mg/dL).
Nephrotic Syndrome, on the other hand, involves massive leakage of protein. Symptoms include:
- Proteinuria exceeding 3.5 grams per day.
- Low albumin levels in the blood (below 3.0 g/dL).
- Severe swelling, especially in the abdomen and legs.
- High cholesterol levels (LDL often >160 mg/dL).
Some forms of glomerulonephritis show features of both. For instance, Membranoproliferative Glomerulonephritis (MPGN) can present with mixed symptoms, making diagnosis tricky without specialized testing.
Common Types of Glomerulonephritis
Not all cases are created equal. There are several specific types, each with its own cause and progression. Here’s a breakdown of the most common ones:
| Type | Cause/Mechanism | Key Characteristic | Progression Risk |
|---|---|---|---|
| IgA Nephropathy | Immune complex deposition (IgA) | Most common primary GN worldwide | 20-40% progress to kidney failure over 20 years |
| Post-Streptococcal GN | Infection-triggered (strep throat/skin) | Common in children; often resolves spontaneously | 95% recovery rate within 6-8 weeks |
| Lupus Nephritis | Autoimmune (SLE-related) | Affects 50-60% of SLE patients | 70-80% renal survival at 10 years with treatment |
| C3 Glomerulonephritis (C3G) | Complement system dysregulation | C3 protein accumulates in glomeruli | High risk of progression if untreated |
| Membranous Nephropathy | Antibody attack on podocytes | Causes nephrotic syndrome in adults | Variable; some resolve, others progress slowly |
IgA Nephropathy is the most frequent form globally. It often flares up after respiratory infections. While many people live with it for decades without major issues, about a quarter will eventually face end-stage renal disease. Post-streptococcal GN is different-it’s an acute reaction to a strep infection. Kids get it most often, and the good news is that most recover completely on their own within two months. Lupus Nephritis is part of systemic lupus erythematosus (SLE). Since lupus affects the whole body, the kidney involvement can be severe, requiring aggressive immunosuppression.
Diagnosis: Why a Biopsy Is Often Necessary
If your doctor suspects glomerulonephritis, blood and urine tests are the first step. They’ll look for protein, blood, and markers of kidney function like creatinine and eGFR. But here’s the catch: these tests tell you *that* something is wrong, not *what* specifically is causing it.
That’s where a kidney biopsy comes in. It’s the gold standard for diagnosis. A small sample of kidney tissue is removed using a needle guided by ultrasound or CT scan. This allows pathologists to examine the glomeruli under a microscope and even use electron microscopy to see ultrastructural details.
Is it risky? Yes, slightly. The American Society of Nephrology reports a complication rate of 3-5%, mostly involving bleeding or pain. However, the information gained is invaluable. It determines whether you have IgA nephropathy, C3G, or another type, which directly dictates your treatment plan. Without a biopsy, doctors are essentially guessing, which can lead to ineffective or harmful treatments.
Treatment Options: From Steroids to Targeted Therapies
Treating glomerulonephritis isn’t one-size-fits-all. The goal is always twofold: stop the immune attack and preserve kidney function. Here’s what that looks like in practice.
First-Line Therapy: Corticosteroids
For many years, corticosteroids like prednisone have been the go-to treatment. They suppress the immune system broadly. About 60-80% of patients respond initially. But the side effects are real and significant. Weight gain, mood swings, increased infection risk, and bone density loss are common. In fact, the NEPTUNE study found that 72% of patients reported weight gain and 28% experienced bone density loss within the first year.
Immunosuppressants
Often used alongside steroids, drugs like cyclophosphamide, mycophenolate mofetil, or rituximab help reduce the immune response further. Rituximab, for example, targets B-cells, which produce the antibodies driving the attack. Some patients report that starting rituximab early prevented them from needing dialysis later on.
Targeted Complement Inhibitors
This is where things are getting exciting. Newer drugs target specific parts of the immune system rather than shutting it down entirely. For C3 Glomerulonephritis, drugs like eculizumab and iptacopan block the complement cascade. Iptacopan received breakthrough therapy designation from the FDA in 2023 after showing a 52% reduction in proteinuria. However, these treatments come with a hefty price tag-around $500,000 annually-and aren’t accessible to everyone yet.
Supportive Care
Regardless of the specific drug regimen, managing blood pressure and reducing protein intake are crucial. ACE inhibitors or ARBs are commonly prescribed to lower blood pressure and reduce protein leakage. Dietary changes, such as limiting salt and sodium, help control edema and hypertension.
Living with Glomerulonephritis: Patient Perspectives
Medicine gives us the stats, but living with the disease tells the real story. Surveys from the American Kidney Fund reveal that 65% of GN patients struggle with significant fatigue. Many describe it as their most debilitating symptom. Edema (swelling) is another major complaint, mentioned in nearly 80% of patient forum posts.
Diagnosis can be a frustrating journey. On Reddit’s r/kidneydisease community, patients shared that it took an average of 4.2 months from symptom onset to get a definitive diagnosis, with nearly a third seeing three or more specialists before finding answers. Early diagnosis is key. One patient noted that starting targeted therapy within two months saved their kidneys from progressing to dialysis.
However, the road isn’t smooth. Side effects from long-term steroid use, such as osteoporosis and fractures, are a serious concern. One patient shared a harrowing experience of suffering two vertebral fractures within 18 months due to prednisone-induced bone loss. This highlights the importance of monitoring bone health and considering alternative therapies when possible.
Future Directions: Personalized Medicine for Kidney Health
The landscape of glomerulonephritis treatment is shifting rapidly. We’re moving away from broad immunosuppression toward precision medicine. Dr. Richard Lafayette from Stanford University predicts that within five years, genetic and proteomic profiling will guide personalized therapy selection. Imagine knowing exactly which pathway is malfunctioning in your body and targeting only that-potentially increasing treatment efficacy from 60-70% to over 85%.
The European Renal Association’s 2023 guidelines already incorporate molecular biomarkers alongside traditional histopathology, improving prediction accuracy for treatment response. Yet, access remains a huge issue. Patients in low-income countries have significantly less access to advanced diagnostics and novel therapeutics, creating a global disparity in outcomes.
Research continues to focus on podocyte repair mechanisms. If we can teach these cells to heal themselves instead of just stopping the attack, we could change the course of the disease entirely. Until then, early detection, accurate diagnosis via biopsy, and tailored treatment remain our best tools.
What are the first signs of glomerulonephritis?
The earliest signs often include changes in urine appearance (pink, red, or brown color due to blood), foamy urine (indicating protein), and swelling in the legs, ankles, or around the eyes. You might also experience high blood pressure or fatigue. If you notice these symptoms, especially after a recent infection, see a doctor promptly.
Is glomerulonephritis curable?
It depends on the type. Post-streptococcal glomerulonephritis often resolves completely on its own. Other types, like IgA nephropathy or Lupus Nephritis, are chronic conditions that can be managed but not necessarily cured. The goal of treatment is to slow progression and preserve kidney function. With modern therapies, many people live normal lives with stable kidney health.
Do I need a kidney biopsy to diagnose glomerulonephritis?
In most cases, yes. While blood and urine tests can suggest kidney inflammation, a biopsy is the only way to determine the exact type of glomerulonephritis. This distinction is critical because different types require vastly different treatments. Skipping a biopsy might lead to ineffective therapy.
Can diet help manage glomerulonephritis?
Diet plays a supportive role. Limiting sodium helps control blood pressure and swelling. Reducing protein intake may ease the workload on damaged kidneys. However, diet alone cannot stop the immune attack. It should always be combined with medical treatment prescribed by your nephrologist.
What are the side effects of steroid treatment for GN?
Common side effects include weight gain, moon face, acne, mood swings, increased appetite, and insomnia. Long-term use raises the risk of infections, osteoporosis (bone thinning), diabetes, and cataracts. Doctors try to taper doses quickly once the inflammation is under control to minimize these risks.
How fast does glomerulonephritis progress?
Progression varies wildly. Acute forms like post-streptococcal GN can resolve in weeks. Chronic forms like IgA nephropathy may take 10-20 years to reach end-stage renal disease, if they do at all. Regular monitoring of urine protein and kidney function (eGFR) helps track progression and adjust treatment early.