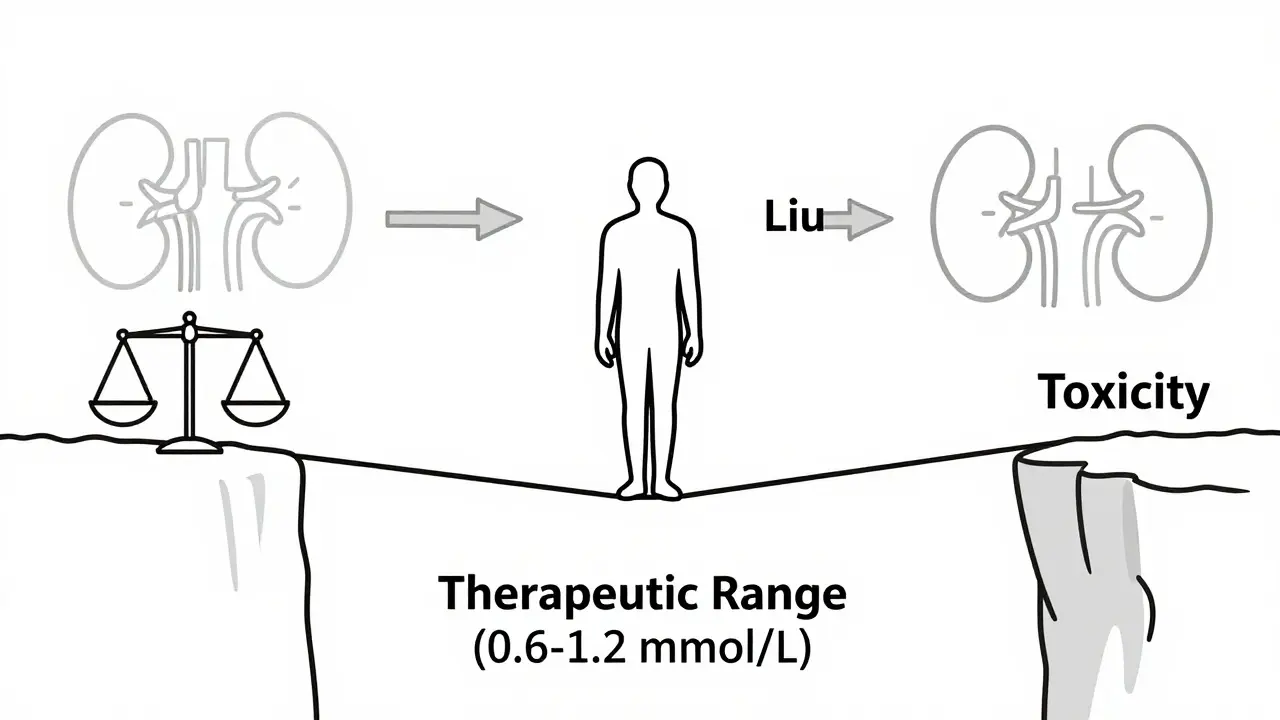
You take your Lithium is a mood stabilizer medication primarily used to treat bipolar disorder by regulating neurotransmitter activity in the brain. It has been a cornerstone of psychiatric treatment since its FDA approval in 1970 and helps millions maintain emotional stability. daily because it keeps your mood stable. But here is the catch: Lithium sits on a razor-thin line between helping you and hurting you. The therapeutic window-the safe range where the drug works without causing harm-is incredibly narrow, typically sitting between 0.6 and 1.2 mmol/L. Go slightly above that, and you risk toxicity. And you don’t need a massive overdose to cross that line. Sometimes, all it takes is a simple painkiller for a headache or a change in your water intake.
This article breaks down exactly which common medications and lifestyle factors can spike your lithium levels, how to spot the early warning signs of trouble, and what steps you can take right now to stay safe. We are looking at the big three risks: NSAIDs (like ibuprofen), diuretics (water pills), and dehydration.
The Narrow Therapeutic Index: Why Small Changes Matter
To understand why these interactions are so dangerous, you first have to look at how your body handles lithium. Unlike most drugs that get broken down by the liver, your kidneys handle almost all of it. About 95% of the lithium you ingest leaves your body unchanged through urine. This makes lithium uniquely sensitive to anything that affects kidney function or fluid balance.
Think of your kidneys like a filter. When they work normally, they let excess lithium pass out. But if something slows down that filtration process-whether it’s a medication, low salt intake, or lack of water-lithium starts to build up in your blood. Because the margin for error is so small, even a 25% increase in lithium concentration can push you from "therapeutic" into "toxic."
This sensitivity is why age matters significantly. Patients over 65 face a 3.2 times higher risk of lithium toxicity compared to younger adults. Their kidneys naturally filter less efficiently, and they often take other medications that compound the risk. If you are older, or if you have existing heart or kidney conditions, this interaction risk is not just theoretical-it is a daily reality you must manage actively.
NSAIDs: The Hidden Danger in Your Medicine Cabinet
Non-steroidal anti-inflammatory drugs (NSAIDs) are everywhere. You reach for them when your back hurts, after a workout, or when you have a migraine. Common names include ibuprofen (Advil, Motrin), naproxen (Aleve), and indomethacin. For someone taking lithium, these drugs are particularly tricky because they interfere with how your kidneys filter blood.
Here is the mechanism: NSAIDs block the production of prostaglandins, chemicals that help keep blood vessels in the kidneys dilated. When those vessels constrict, the glomerular filtration rate (GFR) drops. Since lithium relies on GFR to exit the body, a drop in filtration means lithium stays in your system longer. Studies show that NSAIDs can decrease lithium clearance by 25% to 50%, depending on the specific drug.
| Medication | Estimated Increase in Lithium Levels | Risk Level |
|---|---|---|
| Indomethacin | 30-60% | Very High |
| Ibuprofen | 25-40% | High |
| Celecoxib | 15-30% | Moderate |
| Naproxen | Variable (often high) | High |
As you can see, indomethacin is the worst offender, potentially spiking lithium levels by up to 60%. Ibuprofen, which many people consider harmless, can still raise levels by nearly half. The danger isn't just in chronic use; even short-term courses can cause issues within the first week of starting an NSAID. Experts generally advise avoiding regular NSAID use while on lithium. If you must take one for acute pain, do so under medical supervision with close monitoring of your lithium levels.
A safer alternative for occasional pain relief is acetaminophen (Tylenol/Paracetamol). Acetaminophen does not affect kidney prostaglandins in the same way, meaning it does not significantly alter lithium clearance. Keep a bottle of this on hand instead of reaching for ibuprofen.
Diuretics: Water Pills and Lithium Retention
If you have high blood pressure, your doctor might prescribe a diuretic. These medications help your body get rid of excess salt and water. Unfortunately, when your body tries to hold onto sodium due to diuretic use, it also holds onto lithium. This is because lithium mimics sodium in the kidneys. When the kidneys reabsorb sodium to compensate for the diuretic, they accidentally reabsorb lithium too.
Not all diuretics are created equal, however. Thiazide diuretics, such as hydrochlorothiazide (HCTZ), are the most problematic. They can cause serum lithium concentrations to rise rapidly-by 25% to 50%-within just 7 to 10 days. This rapid spike often leads to toxicity before patients even realize there is a problem.
Loop diuretics, like furosemide (Lasix), pose a lower but still significant risk. They tend to increase lithium levels by only 10% to 25%, making them a slightly safer option if a diuretic is absolutely necessary. Potassium-sparing diuretics like spironolactone show variable effects, with limited evidence on their exact impact.
Interestingly, some diuretics actually lower lithium levels. Osmotic diuretics (like mannitol) and carbonic anhydrase inhibitors (like acetazolamide) can decrease lithium concentrations by 15% to 30%. While this sounds good, it creates a different risk: sub-therapeutic levels, meaning your bipolar disorder might not be controlled effectively. Balance is key, and any change in diuretic therapy requires immediate communication with your psychiatrist.
Dehydration and Sodium: The Silent Multipliers
Medications aren't the only things that shift your lithium levels. Your physiology plays a massive role. Dehydration is perhaps the most common trigger for lithium toxicity outside of prescription errors. Lithium levels rise proportionally when the amount of water in your blood decreases. Even mild dehydration-losing just 2% to 3% of your body weight in fluids-can increase lithium concentrations by 15% to 25%.
Consider these scenarios:
- Summer travel: Sweating more than usual without replacing fluids.
- Gastroenteritis: Vomiting or diarrhea leads to rapid fluid and salt loss.
- Intense exercise: Heavy sweating without adequate hydration.
- Fever: Increased metabolic rate and fluid loss.
In these situations, your kidneys go into conservation mode. They try to save every drop of water and salt, which means they retain lithium aggressively. The NHS Borders guidelines explicitly warn that patients should maintain high fluid intake, especially during illness or hot weather. If you are sick with the flu or food poisoning, do not simply skip your lithium dose without consulting your doctor. Instead, focus on aggressive rehydration with electrolyte solutions, but be aware that your lithium level may still fluctuate.
Sodium intake is equally critical. Lithium and sodium compete for absorption in the kidneys. If you eat a very low-salt diet, your kidneys reabsorb more lithium, raising blood levels. Conversely, a sudden high-salt meal can flush lithium out, lowering your levels and potentially triggering a mood episode. Aim for consistency. Do not switch to a strict low-sodium diet overnight without telling your prescriber. A change of just 20-30 mmol/day in sodium intake can alter lithium concentrations by 10-20%.
Recognizing Lithium Toxicity Early
You cannot wait for a lab test to tell you if you are in trouble. You need to know your body. Lithium toxicity progresses in stages, and catching it early can prevent permanent damage. The earliest symptoms are often mistaken for minor ailments or side effects of the medication itself.
Watch for these red flags:
- Gastrointestinal distress: Nausea, vomiting, and diarrhea are reported in 68% of early toxicity cases. If you suddenly develop stomach issues, check your lithium level immediately.
- Neurological changes: Fine tremors in your hands may become coarse or shaky. Lightheadedness and drowsiness occur in over half of early cases.
- Sensory disturbances: Blurred vision and tinnitus (ringing in the ears) are signs of moderate toxicity.
- Cognitive fog: Difficulty concentrating, slurred speech, or confusion.
If these symptoms progress untreated, severe toxicity can lead to seizures, coma, and permanent renal impairment. There was a documented case of a 72-year-old woman who died from lithium toxicity after adding an NSAID to her regimen while also taking an ACE inhibitor. Her levels were only monitored sporadically. This tragedy highlights that vigilance is non-negotiable.
Practical Safety Strategies for Daily Life
Living safely on lithium doesn't mean living in fear. It means being proactive. Here is a checklist to keep you protected:
- Standardize your labs: Check your lithium levels regularly. If you start a new medication like an NSAID or diuretic, check again within one week, then weekly for the first month.
- Hydrate intentionally: Drink water consistently throughout the day. Don't wait until you are thirsty. During summer or illness, increase intake proactively.
- Stick to acetaminophen: Make paracetamol your go-to for pain and fever. Avoid ibuprofen and naproxen unless cleared by your doctor.
- Communicate with all providers: Tell your dentist, GP, and any specialist that you are on lithium. Many doctors forget to ask about psychiatric meds, leading to dangerous prescriptions.
- Monitor salt intake: Keep your dietary sodium consistent. Avoid extreme diets like keto or strict low-salt regimens without medical oversight.
- Travel smart: If you are flying long distances or traveling to hot climates, carry extra water and electrolytes. Inform your doctor beforehand so they can adjust your dose if needed.
Remember, lithium is a powerful tool for managing bipolar disorder, but it demands respect. By understanding how NSAIDs, diuretics, and dehydration interact with this medication, you take control of your health. You don't have to guess; you have data. Use it to stay stable, safe, and well.
Can I take ibuprofen if I am on lithium?
It is generally advised to avoid ibuprofen while taking lithium. Ibuprofen can increase lithium levels by 25-40%, raising the risk of toxicity. Acetaminophen (paracetamol) is a safer alternative for pain relief. If you must take ibuprofen, consult your doctor first and monitor your lithium levels closely.
How quickly do NSAIDs affect lithium levels?
The interaction between NSAIDs and lithium can occur within the first week of starting the NSAID. In some cases, especially in elderly patients or those who are dehydrated, the rise in lithium levels can happen even faster. Regular monitoring is essential during this period.
What are the first signs of lithium toxicity?
Early signs include nausea, vomiting, diarrhea, fine hand tremors, lightheadedness, and drowsiness. As toxicity worsens, you may experience blurred vision, ringing in the ears (tinnitus), confusion, and slurred speech. Seek medical attention immediately if you notice these symptoms.
Do all diuretics interact with lithium?
Most diuretics increase lithium levels, but the severity varies. Thiazide diuretics (like hydrochlorothiazide) cause the most significant increases (25-50%). Loop diuretics (like furosemide) have a milder effect (10-25%). Some diuretics, like acetazolamide, may actually lower lithium levels. Always inform your doctor if you are prescribed a diuretic.
How does dehydration affect lithium levels?
Dehydration causes the kidneys to conserve water and salt, which leads to increased reabsorption of lithium. Even mild dehydration (2-3% body weight loss) can raise lithium levels by 15-25%. Maintain consistent fluid intake, especially during hot weather, exercise, or illness.
Is it safe to stop lithium if I feel unwell?
No, never stop lithium abruptly without consulting your doctor. Stopping suddenly can trigger a severe mood episode or withdrawal symptoms. If you suspect toxicity due to illness or new medication, contact your healthcare provider for guidance on whether to adjust the dose temporarily.