For many people with rheumatoid arthritis (RA), the dream isn't just managing pain-it's getting to a point where the disease is quiet, joints don't swell, and mornings don't start with stiffness. That point is remission. And the most proven way to get there isn't guesswork or waiting to see what happens-it's treat-to-target (T2T). This isn't a new fad. It's a science-backed, step-by-step plan that's changed how RA is treated worldwide. If you or someone you care about has RA, understanding this approach could mean the difference between lifelong pain and living well.
What Treat-to-Target Really Means
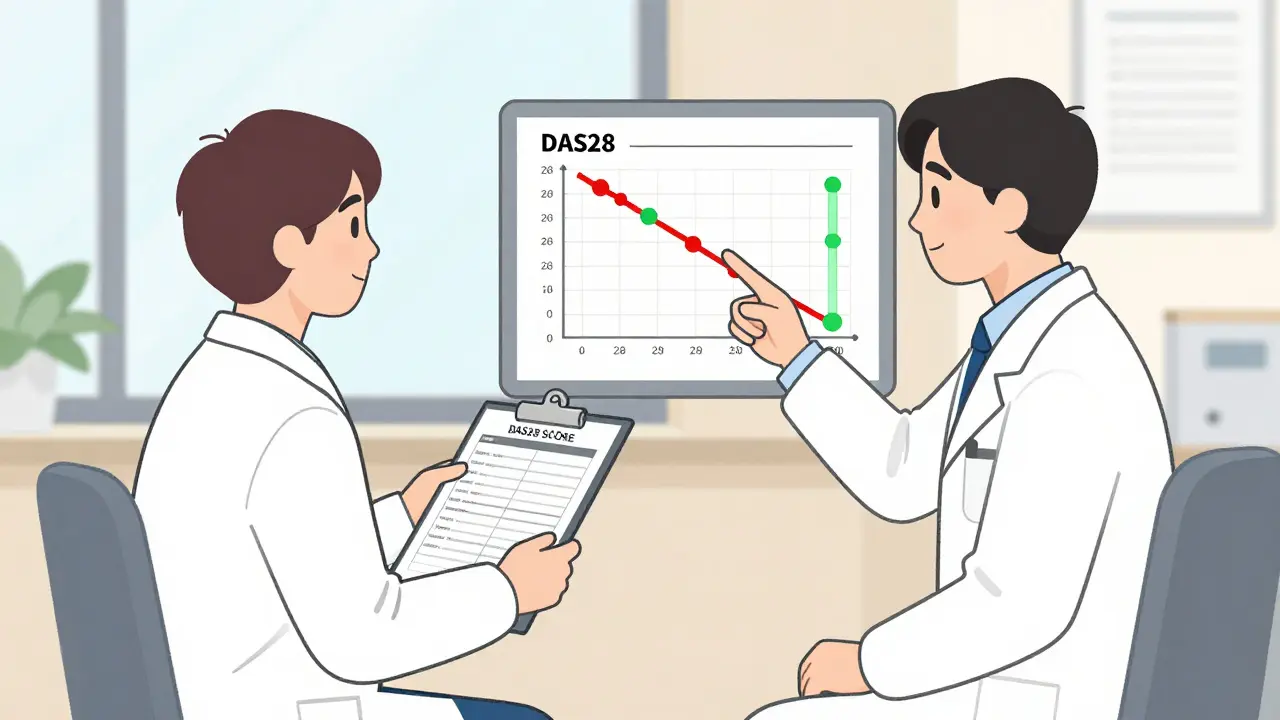
Treat-to-target isn't about hoping things get better. It's about setting a clear goal-remission or low disease activity-and then checking progress every few weeks, not every few months. Think of it like managing diabetes: you don't wait until you feel awful to check your blood sugar. You measure, adjust, and repeat. With RA, the target is usually a score called DAS28. If it's below 2.6, you're in remission. Between 2.6 and 3.2? You're in low disease activity. That's the goal.
Before T2T, doctors often adjusted meds based on how you felt or how bad your joints looked at a single visit. But feelings lie. Swelling can hide. That's why studies like the Dutch DREAM trial, which followed over 500 patients starting in the early 2000s, changed everything. They proved that when you measure disease activity every 1-3 months and change treatment if you're not hitting the target, remission rates jump from 28% to nearly 60%. That’s more than double.
The Science Behind the Strategy
The evidence isn't just from one study-it's from dozens. The BeSt trial showed 61% of patients reached remission after two years using T2T. The TICORA trial found 47% remission with T2T versus 28% with usual care. And in the CAMERA-II trial, 50% achieved remission at two years compared to just 28% without the structured approach. These aren't small numbers. They're life-changing.
Why does this work? Because RA is a ticking time bomb. Every month of uncontrolled inflammation damages cartilage and bone. The sooner you suppress it, the less damage you get. T2T catches flares early, before they wreck your joints. It also means you're less likely to need joint replacements later. One study found that patients on T2T had 40% less joint damage on X-rays after three years compared to those treated the old way.
And it's not just about joints. People in remission report better sleep, less fatigue, and can actually go back to work or play with their kids. The DREAM study showed sustained improvements in physical function and quality of life that lasted for years.
How T2T Works in Practice
Here's how it looks on the ground:
- You start with methotrexate-the most common first-line drug. Dose is usually 10-25mg per week.
- At your next visit, 6-12 weeks later, your doctor checks your DAS28 score. That means counting 28 joints for swelling and tenderness, plus a blood test for inflammation (CRP or ESR).
- If your score is still above 3.2? You don't wait. You don't hope. You escalate.
- Next step: add another DMARD, like sulfasalazine or hydroxychloroquine. Triple therapy (methotrexate + two others) works well for many.
- If that doesn't get you below 2.6 in 3 months? You move to a biologic or JAK inhibitor.
Biologics like adalimumab, etanercept, or tocilizumab block specific parts of the immune system that drive RA. JAK inhibitors like baricitinib or upadacitinib work inside cells to stop inflammation signals. These aren't last-resort drugs anymore-they're part of the plan, and they work faster when used early.
It's not magic. It's method. And it's fast. In the DREAM trial, patients reached remission in 25 weeks on average-half the time it took without T2T.
Who Benefits Most?
T2T shines brightest in early RA-people who've had symptoms for less than a year. In that group, remission rates jump to over 60% with T2T. But it's not useless for long-term RA. The TEAR trial showed that even after years of disease, 65% of patients on T2T reached low disease activity, compared to 52% with usual care. That's still a big win.
But here's the catch: not everyone reaches remission. And that's okay. Some people do better with low disease activity. The 2022 EULAR guidelines now say: your target should be personal. If you're a single parent who needs to be able to pick up your child every day, maybe low disease activity is enough. If you're a marathon runner, maybe remission is non-negotiable. The goal isn't perfection-it's function.
Why It's Not Working Everywhere
Here's the ugly truth: even though T2T is the gold standard, it's not standard practice. A 2022 study found that only 40.8% of rheumatologists and patients even agree on what the treatment goal is. That's not a typo. That's less than half.
Why? Because measuring DAS28 takes time. Counting 28 joints, running blood tests, adjusting meds-it's more work than just writing a prescription. Many clinics don't have the staff, the time, or the EHR systems to automate it. One survey found only 58% of rheumatologists use standardized scores at every visit.
Patients, too, get discouraged. Some feel like failures if they don't hit remission. One user on MyRheumaTeam wrote: "Felt like a failure when I couldn't reach remission despite following all protocols." But remission isn't about willpower. It's about biology, timing, and the right drug sequence. And sometimes, the target shifts.

What You Can Do
If you have RA, here's how to get on the T2T path:
- Ask your rheumatologist: "What's my DAS28 score right now? What's our target?" If they don't know or don't track it, ask why.
- Request a written plan: "What happens if I'm not at target in 3 months?" You deserve to know the next steps.
- Track your own symptoms. Use a simple app or notebook. Note morning stiffness, pain levels, fatigue. This helps your doctor see patterns.
- Don't stop meds just because you feel better. Remission doesn't mean cured. Stopping treatment too soon can trigger a flare.
- Ask about support tools. The ACR has a free "Treat to Target" app. The EULAR toolkit has printable guides in 12 languages.
And if your doctor says, "We'll just monitor," push back. You have the right to a plan. Remission is possible. But it won't happen by accident.
The Future of T2T
What's next? Digital tools. The DART trial is testing a smartphone app that uses your self-reported symptoms, movement data from your phone's sensors, and lab results to predict flares before they happen. Imagine getting a notification: "Your risk of flare is high. Let's adjust your dose." That's not sci-fi-it's coming.
And soon, we may use your genes, your immune cell patterns, even your gut microbiome to pick the right drug before you even start. Dr. Iain McInnes, president of EULAR, predicts we'll be using multi-omics data to tailor treatment within five years. That means less trial and error, and more precision.
But the core won't change: measure, adjust, repeat. That's the heart of T2T. And for millions with RA, it's the difference between surviving and living.
Can rheumatoid arthritis really go into remission?
Yes. Remission means little to no disease activity-no joint swelling, minimal pain, and normal function. Studies show that with treat-to-target strategies, 47% to 68% of patients reach remission within a year, especially if treatment starts early. It's not guaranteed for everyone, but it's far more likely with structured care than with casual management.
What is DAS28, and why does it matter?
DAS28 is a score that measures rheumatoid arthritis activity by checking 28 joints for swelling and tenderness, plus a blood test for inflammation (CRP or ESR). It's the most common tool used in treat-to-target. A score below 2.6 means remission; 2.6-3.2 means low disease activity. It's objective, repeatable, and proven to predict long-term outcomes like joint damage and disability.
How often should I be checked if I'm on T2T?
When your disease is active, you should be assessed every 1 to 3 months. Once you reach your target (remission or low disease activity), checks can slow to every 3 to 6 months. Skipping visits or delaying tests is one of the biggest reasons T2T fails in real life. Consistency is key.
Are biologics and JAK inhibitors dangerous?
All medications carry risks. Biologics and JAK inhibitors can increase the chance of infections or, rarely, certain cancers. But for most people with active RA, the risk of joint destruction, heart disease, and disability from uncontrolled inflammation is far greater. Doctors screen for risks before starting these drugs and monitor closely. For many, the benefits far outweigh the risks.
What if I can't reach remission?
Low disease activity is still a win. The goal of T2T isn't perfection-it's function. If you can move without pain, sleep through the night, and do your daily tasks, that's success. Some people need to adjust their target. A 2022 update to EULAR guidelines says your goal should match your life. Maybe you don't need to be symptom-free-you just need to be able to care for your family or hold a job. That's valid.
Is T2T only for people in wealthy countries?
No, but access is unequal. In Western Europe and North America, over 65% of rheumatologists use T2T. In low- and middle-income countries, it's below 25% due to lack of testing tools, expensive drugs, and few specialists. Researchers are now developing simplified versions-like using just joint counts and patient-reported pain-to make it work where labs and biologics aren't available. The principle-measure, adjust, repeat-can be adapted.
All Comments
Milad Jawabra March 4, 2026
This is the kind of info that actually saves lives. I've seen friends go from barely walking to hiking mountains because they finally got on T2T. Stop treating RA like it's just 'bad days' - it's an autoimmune war and you need a battle plan. 🚀
Zacharia Reda March 6, 2026
So let me get this straight... you're telling me if I just *check my joints* and *adjust meds* instead of waiting until I'm crying in the shower, I could actually feel normal again? Wow. The medical system really does love to keep people suffering for brand loyalty, huh?
Jeff Card March 6, 2026
I was diagnosed 8 years ago and spent the first 5 years being told 'it's just part of living with RA.' Then my rheum started using DAS28 every 6 weeks. Within 4 months, I could hold my granddaughter without wincing. This isn't hype - it's science that works. Thank you for laying it out so clearly.
Matt Alexander March 7, 2026
Methotrexate first. Then if it's not working in 3 months, add something else. If still no progress, go biologic. No waiting. No 'let's see how you feel.' That's it. Simple. Done right, it works.
Gretchen Rivas March 9, 2026
I'm a nurse. I've seen patients who hit remission and cry because they forgot what it felt like to wake up without pain. T2T isn't just medical - it's emotional healing.
Donna Zurick March 11, 2026
I hit remission at 27 after 3 years of trying everything and my doctor finally went full T2T. I'm back to running 5Ks. No drama. Just science. If you're not doing this, you're doing yourself dirty
Tobias Mösl March 13, 2026
Let's be real - Big Pharma loves T2T because it keeps you on expensive biologics for life. They don't care if you're in remission, they care if you're on their drug. This 'strategy' is just a profit pipeline wrapped in science jargon. Ask yourself: who benefits?
tatiana verdesoto March 14, 2026
I used to think remission meant I had to be perfect. Then I realized - I just needed to be able to carry groceries without my hands screaming. Low disease activity? That’s my win. And I’m proud of it. 🤍
Darren Torpey March 16, 2026
T2T didn't just change my joints - it changed my whole life. I went from hiding under blankets to coaching my kid's soccer team. It's not about being 'cured.' It's about getting your damn life back. And yeah - it's possible.
Lebogang kekana March 17, 2026
In South Africa, we don't have biologics. But we have joint counts. We have patient logs. We have community health workers who call every 2 weeks. We don't need fancy labs to measure progress. We just need someone who cares enough to ask: 'How are you really doing?'
Justin Rodriguez March 19, 2026
I’ve been on T2T for 4 years. I still have bad days. But now I know what to do. My rheum says: 'If your DAS28 goes above 3.2, we tweak. No waiting.' That consistency? That’s the magic. Not the drug. The discipline.
Raman Kapri March 20, 2026
The claim that T2T achieves 60% remission is statistically misleading. Many trials exclude patients with comorbidities, non-adherent populations, or those over 65. Real-world outcomes are significantly lower. The data is cherry-picked to sell hope.
Tildi Fletes March 20, 2026
It is imperative to underscore that the operationalization of treat-to-target protocols necessitates a robust infrastructure, including longitudinal biomonitoring, standardized clinical metrics, and consistent patient engagement. Without these foundational elements, the efficacy of such interventions remains theoretically compelling but empirically tenuous.
Siri Elena March 21, 2026
Oh honey, you think *this* is revolutionary? My rheum started doing this in 2009. You're 15 years late to the party. And yes, I still get the 'I'm not sick enough' comment from my insurance. Classic.
RacRac Rachel March 23, 2026
I got my first remission at 32. Took 18 months. Had to switch meds 3 times. But I did it. Now I’m 37, hiking, dancing, and I don’t need a cane. 💪✨ T2T isn’t a trend - it’s your lifeline. Don’t give up.