You’ve been told to use it for your eczema or psoriasis flare-up. It works fast. The redness fades, the itching stops. But then you hear the warning that keeps many of us up at night: skin thinning. Is this powerful medication actually damaging your skin? Or is the fear stopping you from getting the relief you need?
The truth is somewhere in the middle. Topical corticosteroids are among the most effective tools dermatologists have. They are safe when used correctly, but they carry real risks if misused. The key isn’t avoiding them-it’s understanding exactly how to apply them, where to put them, and when to stop.
Understanding Potency and Vehicle Types
Not all steroid creams are created equal. In fact, using the wrong strength for the wrong body part is the fastest way to trigger side effects like thinning skin, stretch marks, or visible blood vessels.
Your doctor will likely prescribe a specific class based on your condition. For thick skin on your palms or soles, a stronger steroid might be necessary. For delicate skin on your face or groin, only mild options should ever be considered. Using a Class I steroid on your eyelids can lead to serious issues like glaucoma or cataracts over time.
The vehicle-the form the medicine comes in-also changes its effectiveness. An ointment is greasy and occlusive, making it more potent than a cream. Creams are better for moist or weeping lesions because they absorb quickly. Gels and lotions work well for hairy areas or flexural zones like behind the knees. Foams are often preferred for the scalp because they don’t leave a heavy residue. Choosing the right vehicle ensures the medicine stays where it needs to work without causing unnecessary irritation.
| Vehicle Type | Potency Level | Best For | Absorption Speed |
|---|---|---|---|
| Ointment | Highest | Dry, thickened skin (palms, soles) | Slow, high retention |
| Cream | Moderate | Moist or weeping lesions | Medium |
| Gel/Lotion | Lower | Hairy areas, flexural zones | Fast |
| Foam | Variable | Scalp, large body areas | Fast, non-greasy |
Measuring Doses with Fingertip Units
One of the biggest reasons people develop side effects is applying too much-or too little. Under-applying prolongs the treatment time, which ironically increases the risk of long-term damage because the inflammation never fully resolves. Over-applying floods the skin, increasing systemic absorption and local thinning.
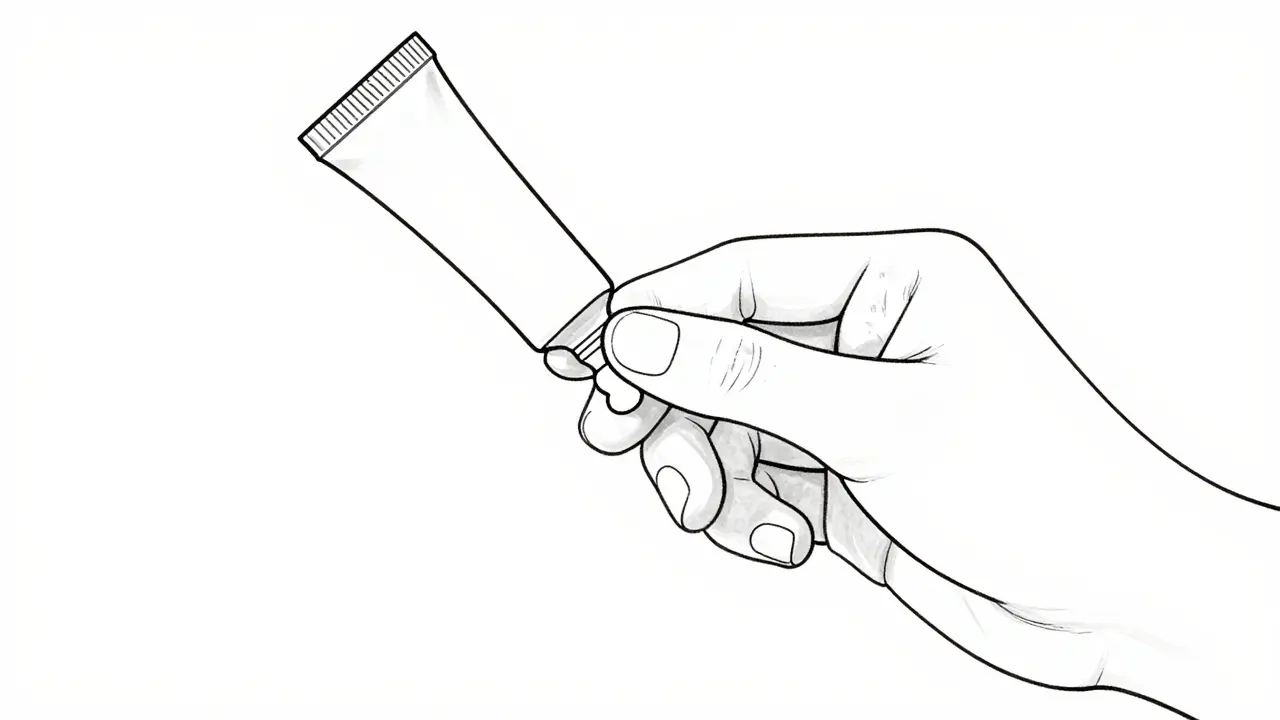
The solution is the Fingertip Unit (FTU). This is a standardized measure that helps you apply the exact amount needed. One FTU is the amount of cream squeezed out from the tip of your adult index finger to the first crease. Depending on the source, this equals approximately 0.25 to 0.5 grams of product. While there is slight variation in medical literature, the visual guide remains consistent.
- One hand (front and back): Requires 1 FTU.
- One arm: Requires 3 FTUs.
- One leg: Requires 6 FTUs.
- One foot: Requires 2 FTUs.
If you’re treating a small patch on your elbow, you don’t need an entire tube. A pea-sized amount is often enough. Learning to estimate these amounts prevents waste and reduces the chance of overdose. If you find yourself running through a tube in three days, you’re likely using too much.
Application Frequency and Timing
How often should you apply the steroid? Contrary to popular belief, more is not better. Research from the American Academy of Family Physicians indicates that applying topical corticosteroids more than once daily for atopic dermatitis provides no additional benefit. In fact, it only raises the risk of adverse effects.
Super-potent to moderately potent steroids (Classes 1-4) are typically applied once daily. Lower potency formulations (Classes 5-7) may be recommended twice daily, but always follow your prescriber’s instructions. Consistency matters more than frequency. Applying a thin layer every morning is far safer than slathering a thick layer once a week.
Timing also plays a role. Many dermatologists recommend applying steroids immediately after bathing while the skin is still slightly damp. This can enhance absorption. However, if you’re also using emollients (moisturizers), order matters. Apply the steroid first, wait 20-30 minutes, and then apply the moisturizer. Applying them simultaneously dilutes the steroid, reducing its effectiveness and forcing you to use more product to get the same result.
Skin Thinning: Causes and Prevention
Skin thinning, or atrophy, is the most common concern associated with long-term steroid use. It happens when the medication suppresses collagen production in the dermis. This leads to fragile skin that bruises easily, develops visible capillaries (telangiectasia), or forms stretch marks (striae).
This risk is highest when high-potency steroids are used for longer than two weeks. The National Institute of Health’s StatPearls resource emphasizes that total treatment duration should rarely exceed 2-4 weeks, regardless of potency. After this period, the skin needs a break to recover its natural barrier function.
To prevent thinning, doctors often use a “step-down” approach. Start with a stronger steroid to knock out the acute inflammation within the first few weeks. Once the flare is under control, switch to a lower potency steroid or a non-steroidal alternative like a calcineurin inhibitor (e.g., tacrolimus or pimecrolimus). These alternatives do not cause skin thinning and are ideal for maintenance therapy, especially on sensitive areas like the face.
Another strategy is “weekend therapy.” Instead of stopping the steroid abruptly, which can cause a rebound flare, some patients apply it only on Saturdays and Sundays for several months. This maintains control while giving the skin five days a week to heal.
Special Considerations for Sensitive Areas
Your face, groin, and underarms are different from the rest of your body. The skin here is thinner and absorbs medications more readily. Using anything stronger than a mild-potency steroid on these areas is risky.
Facial application requires extra caution. Prolonged use of even mild steroids around the mouth can cause perioral dermatitis-a red, bumpy rash that looks like acne but worsens with steroid use. Around the eyes, prolonged exposure can contribute to glaucoma or cataracts. If you have eye involvement, see an ophthalmologist before applying any topical medication near the lids.
In children, the risk is higher due to their larger surface-area-to-weight ratio. Their skin is also more permeable. Always use the lowest effective potency for the shortest possible time. Never wrap treated areas in plastic or tight bandages unless explicitly instructed by a doctor, as occlusion dramatically increases absorption and side effect risks.
When to Seek Help
If you notice your skin becoming translucent, bruising easily, or developing white streaks, stop the medication and consult your healthcare provider. These are signs of atrophy. Similarly, if you experience withdrawal symptoms-such as intense burning, redness, and swelling after stopping a long-term steroid regimen-you may have developed topical steroid dependence. This is rare but serious and requires medical supervision to taper off safely.
Don’t let fear dictate your treatment plan. Untreated eczema or psoriasis can lead to infections, sleep loss, and significant quality-of-life issues. Topical steroids are safe when respected. Use the right strength, measure your dose, limit your duration, and step down when the flare subsides. Your skin will thank you.
Can topical steroids permanently thin my skin?
In most cases, skin thinning is reversible if caught early. Stopping the medication allows collagen production to resume over several weeks to months. However, severe or prolonged misuse can lead to permanent changes like striae (stretch marks) or persistent telangiectasia. Prevention through proper dosing and duration limits is key.
Is it safe to use topical steroids on the face?
Yes, but only with mild-potency steroids and for short durations (usually less than 5-7 days). Stronger steroids should never be used on the face, especially near the eyes, due to risks of glaucoma, cataracts, and perioral dermatitis. Non-steroidal alternatives like tacrolimus are often preferred for facial maintenance.
What is a Fingertip Unit (FTU)?
An FTU is a standardized measure for applying topical medications. It is the amount of cream squeezed from the tip of an adult index finger to the first crease, roughly 0.5 grams. It helps ensure you apply enough medication to be effective without wasting product or causing overdose.
Should I moisturize before or after applying steroid cream?
Apply the steroid first, then wait 20-30 minutes before applying moisturizer. Applying them together dilutes the steroid, reducing its effectiveness. Moisturizers help repair the skin barrier, but they should not interfere with the active medication’s absorption.
How long can I use a potent topical steroid?
Potent and super-potent steroids should generally not be used for more than 2 weeks continuously. Total treatment duration for any potency should rarely exceed 2-4 weeks. Long-term management usually involves stepping down to lower potency or switching to non-steroidal agents.